Cell cycle analysis by quantitation of DNA content was one of the fantastic applications of flow cytometry.
The mammalian DNA, yeast, DNA, plant DNA or bacterial DNA can be easily stained by a variety of DNA binding dyes such as propidium iodide.
The premise of these DNA binding dyes is that they are stoichiometric, i.e. they bind in proportion to the DNA amount present in the cell.
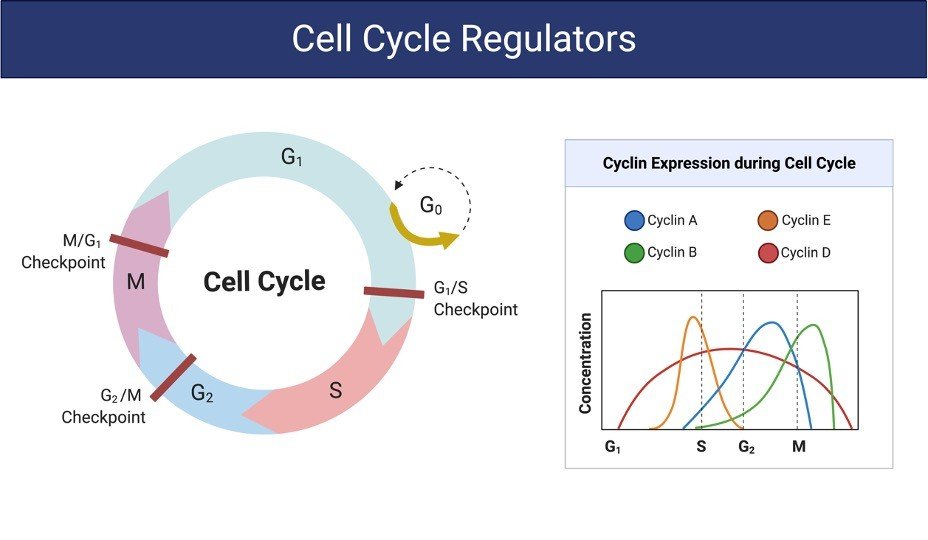
In this way if cells are in S phase will have more DNA than cells in G1 phase.
They will take up proportionally more dye and will fluoresce more brightly until they have doubled their DNA content.
The cells in G2 phase will be approximately twice as bright as cells in G1. DNA-binding dyes include propidium iodide (PI), Hoechst 33342, 33258 and S769121, 7-aminoactinomycin-D (7-AAD), DRAQ5™ and DRAQ7™, TO-PRO-3, 4’6’-diamidino-2-phenylindole (DAPI).
In general, cells must be fixed and permeabilized to allow entry of the DNA binding dye which is otherwise actively pumped out by living cells.
Alcohol or aldehyde are commonly used to fix the cells.
Alcohol is a dehydrating fixative which also permeabilizes cells of interest. This will allow easy access of the dye to the DNA and gives good profiles (low coefficient of variation, CV).
The disadvantage of alcohol fixation is that it is often incompatible with fluorescent proteins and some surface markers.
For simultaneously proteins or surface markers examination, use of an aldehyde (cross-linking) fixative, such as paraformaldehyde is more efficient and appropriate.
Aldehyde fixation in cell cycle analysis may lead to poorer quality profiles (higher CVs) but will allow simultaneous detection of other fluorochromes and membrane-bound surface proteins.
Another disadvantage of paraformaldehyde fixation is, generally paraformaldehyde does not permeabilize the cell membrane, and so further sample processing is required.
With fixed cells, samples may be processed, stained and analyzed at the conclusion of an experiment.
Alcohol-fixed cells are stable for several weeks at 4°C and several weeks in -20 °C.
Aldehyde fixed cells are stable for 2 to 3 days. An alternative method to allow the DNA dye into the cells is to permeabilize them with a detergent such as Triton X-100 (0.1%) or NP40 (0.1%).
Usually, it is also necessary to combine a fixation (paraformaldehyde) and permeabilization (Triton X-100) for the intracellular staining.
On the other hand, methods are available, e.g. use of citrate buffers (in combination with detergent), although these are not so widely used.
There are also some dyes that will enter live cells and quantitatively bind to DNA, these include Hoechst 33342, DRAQ5™ (ab108410) and the DyeCycle dyes